
CONTENTS
Why Care Coordination Software Matters
Benefits of Care Coordination Software
Challenges in Adopting Care Coordination Software and How to Address Them
How Sigma Software Builds Custom Care Coordination Solutions
Thank you for reaching out to Sigma Software!
Please fill the form below. Our team will contact you shortly.
Sigma Software has offices in multiple locations in Europe, Northern America, Asia, and Latin America.

USA

Sweden

Germany

Canada

Israel

Singapore

UAE

Australia

Austria

Ukraine

Poland

Argentina

Brazil

Bulgaria

Colombia

Czech Republic

Mexico

Portugal

Romania

Uzbekistan
7 min read
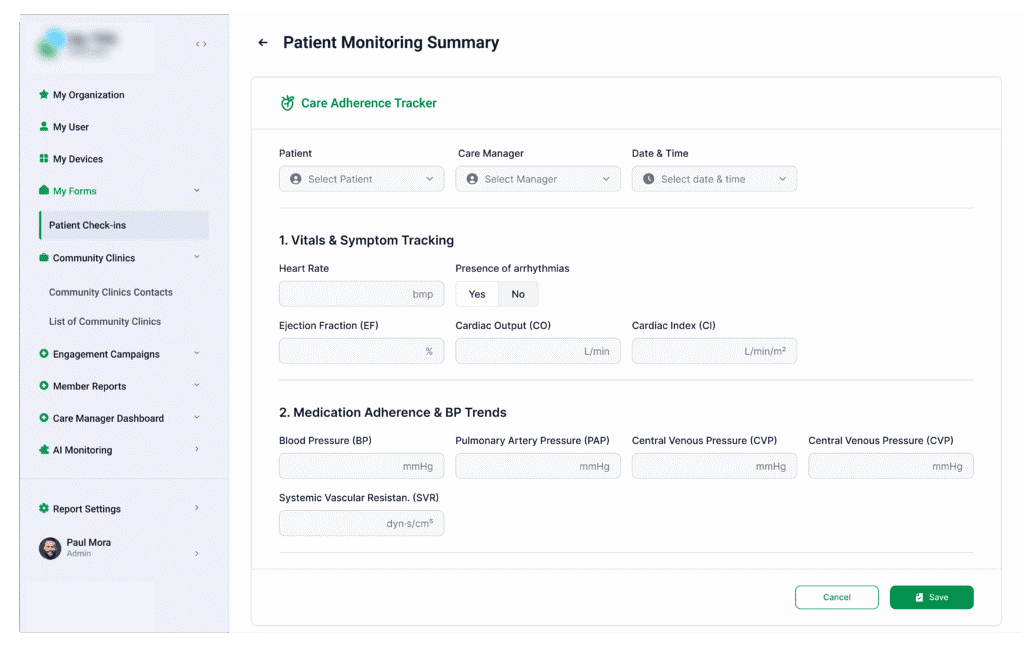
The payment model in healthcare flipped. Volume is out, and outcomes are in. But you cannot improve patient outcomes if the primary care doctor, the specialist, and the payer are all looking at different data. You have to connect the pieces. Right now, care coordination software does exactly that. It pulls patient data into one spot, gets different clinical teams on the same page, handles the messy transitions between facilities, and gives organizations the data they need to hit their contract targets.
Why Care Coordination Software Matters
Benefits of Care Coordination Software
Challenges in Adopting Care Coordination Software and How to Address Them
How Sigma Software Builds Custom Care Coordination Solutions
If you are running an ACO, a hospital, or an insurance plan, you already know the stakes. This guide breaks down why purpose-built coordination platforms fix operational bottlenecks, what goes wrong during rollout, and how to fix those common missteps. We also look at why custom software often beats out rigid, pre-packaged vendors.
Doctors and care managers need access to medical histories, treatment plans, and social factors the second a patient walks in. Having that data ready prevents costly mistakes and speeds up clinical decisions.
Nurses and admins spend way too much time on manual data entry. Setting up automated rules for referrals, scheduling, and follow-ups gets your staff off the phone and back to patient care.
Things go wrong when patients move from the hospital back to their homes. A shared digital record stops duplicate lab tests and keeps the treatment plan intact across different facilities.
You cannot get paid for value if you cannot prove you delivered it. Live dashboards let you track risk scores, readmission rates, and contract compliance daily instead of waiting for a quarterly report.
When care teams communicate consistently, patients actually stick to their treatment plans. Better engagement means better satisfaction scores, which directly impacts payer performance metrics.
Hitting your clinical and financial targets takes software that actually talks to your existing electronic health records (EHRs), claims databases, and lab systems. When the technology fits the workflow, you start to see very specific results:
Read about our service: Remote Patient Monitoring Software for Value-Based Care
Executives know they need better system integration. Actually getting it done is another story. Here are the most common hurdles organizations hit when moving to value-based models, along with practical ways to solve them.
Your teams probably use a mix of different EHRs, claims tools, and telehealth apps. Because these systems store information differently, data gets stuck in silos. Your staff loses hours hunting down patient histories.
The Fix: Smart Integration Layers
You do not need to rip and replace your entire IT setup. The smart move is building a flexible integration layer that connects your new platform with existing databases. Using standard protocols like HL7 and FHIR is the only way to make this work long-term.
Communication usually breaks down when a patient leaves a hospital to go to a specialized rehab facility. Every building uses different paperwork, so care gets delayed.
The Fix: Map the Real Workflow First
Before you write any code, document exactly how your staff handles referrals today. Find out where the data actually drops off. If you build the software to match how your staff naturally works, they will actually use it.
Care managers are drowning in referral tracking and manual quality reporting. All that typing pulls them away from the patients.
The Fix: Automate in Small Bites
Do not try to automate everything on day one. Start with the easy, repetitive stuff: appointment reminders, status updates on referrals, and basic data validation. Taking the pressure off slowly helps your team get comfortable with the new tech.
Sharing data across payer networks and community clinics introduces serious security risks. Throw in social determinants data, and the regulatory side gets incredibly complex.
The Fix: Define clear access rules
Figure out your access policies first. Decide exactly who gets to see what. Then, the software just enforces those rules. You need automated audit logs, encrypted databases, and strict role-based access built in from the start.
If you cannot measure the financial impact of your care managers, you cannot prove the system works. Bad reporting makes it impossible to show improvements in readmission numbers.
The Fix: Define clear access rules
Stop relying solely on high-level summaries. Track daily operational metrics, like how many referrals actually closed or how many social service requests were completed. Put those numbers right on the main dashboard so the team sees their progress every morning.
Money is tight, and your IT team is already underwater. Launching a massive software project sounds like a disaster.
The Fix: Use a phased approach
Skip the massive, system-wide launch. Pick one high-risk patient group or one specific hospital department. Test the software there, fix the bugs, and prove it works before you ask the rest of the organization to change how they work.
Housing, food security, and transportation affect health more than medicine sometimes. Yet, social workers rarely have logins to clinical systems, so vulnerable patients get left behind.
The Fix: Include social care in coordination
Set up the software so doctors can send referrals directly to social service groups. Build mandatory social needs assessments right into the main clinical intake forms so nothing gets skipped.
State programs and ACOs change their reporting rules all the time. Off-the-shelf software is usually too rigid to handle these updates without clumsy workarounds.
The Fix: Build for flexibility
Go with an architecture that administrators can tweak. If a regulation changes, you should be able to update a clinical rule or a reporting field internally. You should never have to pay for a massive codebase rewrite just because a state agency updated a form.
Understanding the realities of value-based care forms the foundation of effective software engineering. Here is a look at the operational approach:
Generic software rarely meets the complex demands of modern healthcare. Instead, custom tools must be engineered to fit actual daily operations and deliver the hard numbers required for payer contracts.
If you are serious about value-based care, you cannot run your operations on disconnected databases and sticky notes. Fragmented workflows hurt patients and bleed money.
Putting money into a custom-built care coordination platform gives you control. It fits your exact security needs, connects your old systems, and matches how your staff actually works. Treating this software as a core piece of your business infrastructure leads directly to better patient health and stronger margins on your payer contracts.

Andrii's expertise primarily encompasses the Healthcare industry. Bolstered by extensive knowledge in the Information Security domain and ML/AI. Andrii Pastushok is committed to guaranteeing clients receive an exceptional product development experience.
Linkedin profile
Most AI assistant deployments start with a question: what can we give this system access to? The more data, the better the answers. That logic is correct – and ...

Biotech executives face a massive data problem. The issue is not gathering information. The issue is making that information useful. Clinical trials slow down b...

Healthcare leaders need to switch from billing for services to getting paid for patient health. Artificial intelligence offers specific tools to manage this shi...